
Limited Access to Research Involving Incarcerated Persons as a Result of Protectionism
Article Sidebar

Main Article Content
Abstract
Photo by Carles Rabada on Unsplash
ABSTRACT
Overall, failure to include incarcerated people in ethically conducted research should not be the standard, as many health-related risks in this population are still unexplored. Fostering participation of incarcerated individuals in ethically conducted research could provide generalizable knowledge to manage chronic disease, mental health, and substance abuse disorders in this unique and high-risk patient population. Moving forward, improvements are required to facilitate the inclusion of incarcerated people in research.
INTRODUCTION
Exploitative research practices have negatively impacted, and even victimized, vulnerable populations. While research ethics frameworks acknowledge that there are “disadvantaged sub-segment[s] of the community, requiring utmost care, specific ancillary considerations, and augmented protections in research,”[1] increased protection has limited the ability of incarcerated individuals to participate in research autonomously and consensually. Protecting vulnerable incarcerated people in this case limits their opportunity compared to other, better-situated populations.
BACKGROUND
The known benefits of research participation for incarcerated individuals are early access to a drug during the trial, a chance to continue the drug even if supply is limited (first in line), and financial compensation. There are also benefits to incarcerated populations as a whole because much research is not easily generalizable to them. Incarcerated people should have access to groundbreaking scientific discoveries and be able to contribute to improving the lives of other incarcerated people. Yet, some argue that because not all scientific research has a positive outcome, research participation places incarcerated people, who are already at risk, at unjustifiably high risk. In other words, they argue that principles of non-exploitation dictate we err on the side of non-inclusion.
Rigorous research protections in the United States originated after World War II, during which Nazi attorneys likened unethical experiments on Jewish people and others to practices common in U.S. correctional facilities.[2] With increased public awareness of research abuses in the wake of the infamous Tuskegee syphilis study, Congress appointed a national commission to create guidelines for research involving vulnerable populations, including the incarcerated.[3] Constituted under the Department of Health, Education, and Welfare (DHEW), the commission produced Report and Recommendations: Research Involving Prisoners (hereinafter the “DHEW Report”).[4] The report recommended that incarcerated people “receive a fair share of the benefits of research,” and encouraged such research to be aimed toward improving “prisoners’ health and/or investigate the causes and effects of incarceration.”[5] These regulations were incorporated into the 1979 Belmont Report and later into the “Common Rule.”[6]
However, many groups representing vulnerable or minority populations, such as women’s rights advocacy and AIDS support groups, requested revisions of the DHEW Report to ensure that a “fair share of the benefits of research” was realized for minority populations, whose interests had not been originally considered.[7] This awareness campaign eventually led the National Institutes of Health (NIH) to loosen restrictions on vulnerable groups’ participation in research of more than minimal risk. Participation became acceptable provided that the improvement of the health of participants or the group was a priority.[8] Currently, research involving incarcerated people must be defined within one of the following four categories:
(1) Minimal-risk studies on possible causes, effects, and processes of incarceration and criminal behavior;
(2) Minimal-risk studies of prisons as institutional structures or of prisoners as incarcerated persons;
(3) Research on conditions particularly affecting prisoners as a class;
(4) Research on practices that are intended and deemed likely to improve the health or well-being of participants.[9]
A recondite fifth category – by means of a HHS Secretarial waiver – grants approval to certain Department of Health and Human Services (HHS) studies solely intended to “(1) describe the prevalence or incidence of a disease by identifying all cases, and (2) study potential risk factors associations for a disease.”[10] Other requirements include limiting risk levels to those comparable for non-incarcerated populations, offering only non-coercive compensation, and the inclusion of a prisoner-representative in the IRB committee.[11]
ANALYSIS
l. Justice and the Opportunity to Participate
These safeguards are vital for ensuring incarcerated peoples’ protection from exploitation and harm.[12] However, when combined with certain state and local measures, they burden the population they are meant to serve by eliminating or severely limiting research opportunities.[13] From 2008 to 2012, no NIH funding was granted to research in California prisons, while Rhode Island DOC (with about only 1 percent of California’s incarcerated population) reported 13 NIH grants totaling $16 million in the same time period.[14] California-based correctional research is restricted by state law that broadly defines and prohibits “biomedical research” on incarcerated people.[15] Meanwhile, Rhode Island has no such state laws.[16]
The U.S. incarcerated population includes a disproportionate number of ethnic and racial minorities, people with mental illnesses, and people with serious infectious diseases like HIV.[17] Barring them from participating in research is discriminatory because they suffer disproportionately from a lack of understanding of their conditions. Other studies may also not easily be generalizable to incarcerated people, who are in a unique environment. Treatment effectiveness in the incarcerated population for many conditions is unknown and thought to be highly variable.[18]
To respect incarcerated peoples’ dignity and “right to science” (more below), a reasonable balance between valuing their autonomy and protecting them from exploitative practices must be found.[19] Over time, a pattern of overprotection has grown, creating a tension between subject protection and scientific progress.[20]
ll. Autonomy and Protection from Coercion
The initial concern about including incarcerated people in research was that prisons are “inherently coercive environments.” Coercion in this context could be exacerbated by financial compensation, the prospect of earlier parole, and even the chance to alleviate boredom.[21] But the incarcerated actively seek participation in research, and this should be recognized. Research outside of prisons is not coercion-free, and within prisons with proper precautions, incarcerated people are able to make autonomous decisions. “As respect for prisoners also requires recognition of their autonomy,”[22] incarcerated people should have many of the same opportunities that others have. It is important to consider incarcerated peoples’ perspectives.
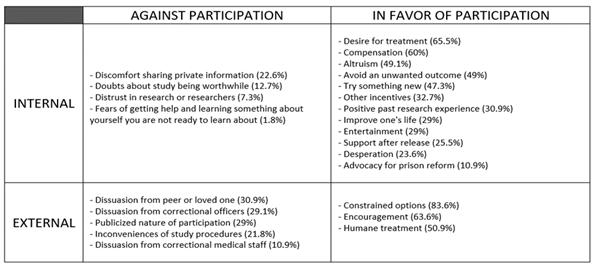
*Chart from: Lerner BH. Subjects or objects? Prisoners and human experimentation. N Engl J Med. 2007 May 3;356(18):1806-7. doi: 10.1056/NEJMp
One study suggested that incarcerated people may not fear involvement in research as much as lawmakers think (only 7.3 percent distrust research or researchers).[23] Instead, it is family members, correctional officers, and nurses who often discourage incarcerated people from joining a study because their participation may create more work for them.[24] Another study found that “few prisoners endorsed feeling exploited by their participation [in research],” and many would like “to participate as a means of gaining access to a treatment that was not readily available to them.”[25] Other people do not accurately represent incarcerated people’s wishes, and their speculation should not be a basis for regulations restricting research participation.
lll. International Human Rights and a Right to Science
The right to science is recognized as a human right in international law.[26] Overprotective research participation policies create novel injustices by blocking access to groundbreaking scientific advances that benefit incarcerated groups.[27] Both the Universal Declaration of Human Rights (UDHR) and the International Covenant on Economic, Social, and Cultural Rights (ICESCR) indicate that every person has the right “to share in scientific advancement and its benefits” and “to enjoy the benefits of scientific progress and its application.”[28] According to Van Westendorp, et al., the right to science, which “must be respected and protected,” consists of four parts:
(1) access by everyone without discrimination to the benefits of science and its applications, including scientific knowledge;
(2) opportunities for all to contribute to the scientific enterprise and freedom necessary to facilitate scientific research;
(3) participation of individuals and communities in decision-making and the related right to information;
(4) and an enabling environment fostering the conservation, development, and diffusion of science and technology.[29]
Despite the existence of international guidelines, the right to science has not been systematically applied at a state level.[30] Overprotective restrictions are unjust, as incarcerated people in some cases are denied the opportunity to reap the benefit of early access to important therapies. Failing to facilitate their inclusion in research limits scientific progress and restricts benefits with respect to the incarcerated population as a whole.[31]
As an example, consider the state of mental healthcare for the incarcerated. A 2012 systematic review identified a high incidence of psychiatric disorders in incarcerated people, especially major depression and psychiatric illnesses, which are related to substance abuse and higher mortality rates.[32] The lack of mental health studies on the incarcerated population prevents knowledge of this special population from reaching physicians in the community where formerly incarcerated people will eventually seek care. It also limits how effectively they are treated when in prison.
lV. How to Improve the System
Moving forward, improvements are required to facilitate the inclusion of incarcerated people in research. One step is to build buy-in from key prison officials. For example, researchers could involve the prison’s Chief Medical Officer and collaborate with prison administrators, potentially listing them as co-investigators on their research studies.[33] Other recommendations include the establishment of an Advisory Council consisting of prison leaders and an Inmate Liaison Committee (ILC) in charge of communicating feedback and updates to inmates.[34] Also, designating a “point person” can help the research team navigate the penitentiary system’s intricacies.[35] These considerations open various communication pathways for incarcerated people. In fact, the appointment of key personnel in charge of working closely with incarcerated people to amplify their voices may be the first necessary step, and it could provide the impetus for yet more change.
For recruitment, it is useful to publish articles in prison newsletters, plan co-authorship with prison staff, use visuals to explain the study, and implement certificates of confidentiality.[36] It is also important to be transparent, not engage in aggressive marketing of the opportunity, and avoid coercion.
CONCLUSION
Overall, failure to include incarcerated people in ethically conducted research should not be the standard, as many health-related risks in this population are still unexplored.[37] Compared to the non-incarcerated population, accessible enrollment of incarcerated people in research studies is not currently being facilitated. They lack access to the internet, cannot look up research opportunities independently due to the inherent nature of their incarceration, and have restricted telephone privileges, etc. Under normal circumstances, the excessive advertising of research opportunities would be considered coercive. However, in a prison setting, implementation of these recruitment strategies may be the only way to inform this vulnerable population about the available research opportunities outside of prison. State legislatures should relax protective regulations when they interfere with autonomy and a right to science. Indeed, there is a delicate line that must be clearly defined to avoid undue coercion, but it is the state leaders’ responsibility to do so to ensure extension of the benefits of science and technology to all parts of the population. Fostering participation of incarcerated individuals in ethically conducted research could provide generalizable knowledge to manage chronic disease, mental health, and substance abuse disorders in this unique and high-risk patient population.
[1] Shivayogi P. (2013). Vulnerable population and methods for their safeguard. Perspectives in clinical research, 4(1), 53–57. https://doi.org/10.4103/2229-3485.106389
[2] Ahalt, C., Haney, C., Kinner, S., & Williams, B. (2018). Balancing the Rights to Protection and Participation: A Call for Expanded Access to Ethically Conducted Correctional Health Research. Journal of general internal medicine, 33(5), 764–768. https://doi.org/10.1007/s11606-018-4318-9
[3] Ahalt, et al.
[4] Ahalt, et al.
[5] Ahalt, et al.
[6] Ahalt, et al.
[7] Ahalt, et al.
[8] Christopher, Paul P., Garcia‐Sampson, Lorena G., Stein, Michael, Johnson, Jennifer, Rich, Josiah and Lidz, Charles, “Enrolling in Clinical Research While Incarcerated: What Influences Participants’ Decisions?” Hastings Center Report 47, no. 2 (2017): 21– 29. DOI: 10.1002/hast.686. Retrieved from https://onlinelibrary-wiley-com.ezproxy.cul.columbia.edu/doi/full/10.1002/hast.686
[9] Christopher, et al.
[10] “Prisoner Research FAQs.” HHS.gov, www.hhs.gov/ohrp/regulations-and-policy/guidance/faq/prisoner-research/index.html
[11] Christopher, et al.
[12] Ahalt, et al.
[13] Ahalt, C., Haney, C., Kinner, S., & Williams, B. (2018). Balancing the Rights to Protection and Participation: A Call for Expanded Access to Ethically Conducted Correctional Health Research. Journal of general internal medicine, 33(5), 764–768. https://doi.org/10.1007/s11606-018-4318-9
[14] Ahalt, et al.
[15] Ahalt, et al.
[16] Ahalt, et al.
[17] Lerner BH. Subjects or objects? Prisoners and human experimentation. N Engl J Med. 2007 May 3;356(18):1806-7. doi: 10.1056/NEJMp068280. PMID: 17476006. Retrieved from https://www-nejm-org.ezproxy.cul.columbia.edu/doi/full/10.1056/NEJMp068280
[18] Mathijs Van Westendorp, Steven Lierman, Walking the Line: Balancing Access to Research and Protecting Prisoners, Medical Law Review, Volume 28, Issue 1, Winter 2020, Pages 65–92, https://doi-org.ezproxy.cul.columbia.edu/10.1093/medlaw/fwy041
[19] Van Westendorp, et al.
[20] Gostin, L. O., Vanchieri, C., Pope, A., & Research, I. of M. (US) C. on E. C. for R. to D. R. for P. of P. I. in. (2007). The Ethical Framework for Research Involving Prisoners. In www.ncbi.nlm.nih.gov. Retrieved from https://www.ncbi.nlm.nih.gov/books/NBK19885/
[21] Lerner BH. Subjects or objects? Prisoners and human experimentation. N Engl J Med. 2007 May 3;356(18):1806-7. doi: 10.1056/NEJMp068280. PMID: 17476006. Retrieved from https://www-nejm-org.ezproxy.cul.columbia.edu/doi/full/10.1056/NEJMp068280
[22] Lerner.
[24] Christopher, et al.
[25] Christopher, et al.
[26] Van Westendorp, et al.
[27] Lerner.
[28] Van Westendorp, Steven Lierman, Walking the Line: Balancing Access to Research and Protecting Prisoners, Medical Law Review, Volume 28, Issue 1, Winter 2020, Pages 65–92, https://doi-org.ezproxy.cul.columbia.edu/10.1093/medlaw/fwy041 (The Charter of Fundamental Rights of the European Union (EU Charter) takes it a step further by stating that “scientific research shall be free of constraints.”)
[29]Van Westendorp, et al.
[30] Van Westendorp, et al.
[31] Van Westendorp, et al.
[32] Fazel, S., Hayes, A. J., Bartellas, K., Clerici, M., & Trestman, R. (2016). Mental health of prisoners: prevalence, adverse outcomes, and interventions. The lancet. Psychiatry, 3(9), 871–881. https://doi.org/10.1016/S2215-0366(16)30142-0
[33] Apa, Z. L., Bai, R., Mukherejee, D. V., Herzig, C. T., Koenigsmann, C., Lowy, F. D., & Larson, E. L. (2012). Challenges and strategies for research in prisons. Public health nursing (Boston, Mass.), 29(5), 467–472. https://doi.org/10.1111/j.1525-1446.2012.01027.x
[34] Apa, et al.
[35] Apa, et al.
[36] Apa, et al.
[37] Ahalt, et al.
Article Details

This work is licensed under a Creative Commons Attribution 4.0 International License.