
Of Free Trade Agreements, Pharmaceuticals and Global Ethics
Article Sidebar

Main Article Content
Abstract
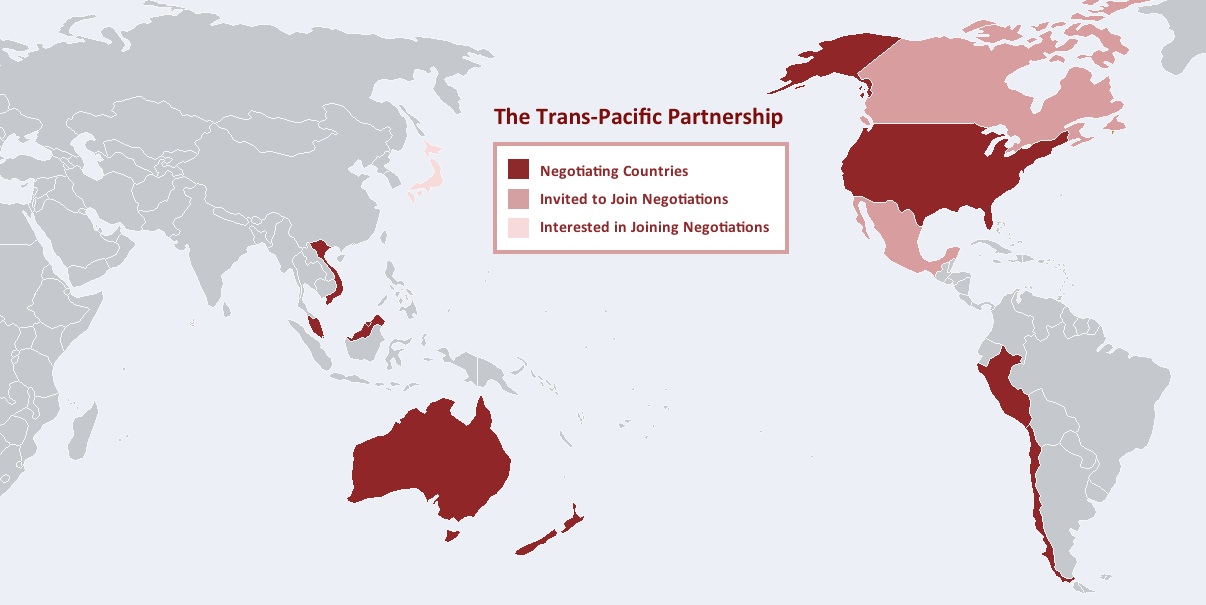
The Trans-Pacific Partnership (TPP) is a proposed multilateral free trade agreement between 12 countries; Australia, Brunei Darussalam, Canada, Chile, Japan, Malaysia, Mexico, New Zealand, Peru, Singapore, USA and Vietnam. The TPP arose out of the Asia-Pacific Economic Cooperation (APEC),and an agreement known as the P4 between Brunei, Chile, Singapore, and New Zealand, a conference with the aim of free and open trade in the Asia-Pacific region. A final round of negotiations was completed in 2013, with some details being closely guarded, and others leaked thanks to whistle-blower Edward Snowden.
Of particular interest for bioethics is how the TPP will handle patent law, intellectual property and pharmaceutical regulation. Focusing on two countries (USA and New Zealand) within the proposed agreement, we can see how varied regulation can have a dramatic impact on cost and thus access to medications.
In 1993 New Zealand created a price regulatory body, the Pharmaceutical Management Agency (PHARMAC), which manages government spending on medicine inside a universal healthcare system. PHARMAC was largely created in response to the astronomical increase in the cost of medicines over the late 1980s and early 1990s. In the first year of implementation, the group achieved savings of $3.1 million and halved the growth in pharmaceutical expenditure to 5 percent per annum. By 2001, cumulative savings passed $1 billion. Recent figures show $937 million saving in the years 2009-10 alone, when compared to a 1999 baseline.
Generally, the PHARMAC system functions well. However, patient dissatisfaction can arise when a relatively rare disease is potentially alleviated with high cost medications. Strict PHARMAC decision criteria are based on nine principles, which encompass population health needs, clinical benefits, direct patient costs and cost-effectiveness of pharmaceutical action over other health interventions. If the potential cost outweighs the benefit, PHARMAC will not fund access to medication. PHARMAC essentially controls what medications and medical devices enter the country and manages pharmaceutical funding for district health boards (DHBs).
The creation of pricing referencing and regulation was not without opposition even in a country with firmly established socialized (universal coverage provided by the government, funded by the taxpayer) healthcare like New Zealand. Early critiques of PHARMAC favored similar arguments as those commonly proposed by fiscally libertarian sides in the US against universal healthcare. A situation where a patient is denied drug access by government regulation due to cost is almost inconceivable in America. Generally in the US, if you can pay for it, you can have it. This ethos stems from an emphasis on individual freedoms propagated through the free market.
The US federal system is designed for less government intervention, and favors a free market economy. Attempts to curtail the dramatic rise in the cost of pharmaceuticals have met with cries of ‘health care rationing’, and claims of devaluing the patent and intellectual property laws that aim to encourage innovation and discovery. The high cost of pharmaceuticals has also been defended on the basis of the high cost of bringing a single drug to market, with one influential (but controversial) study citing a figure of $1.3 billion. As such, regulation of the US pharmaceutical industry comes from within medicine itself; individuals, hospitals or pharmacies, and insurance company funding.
A prime example of this self-regulation in recent years is the decision of Memorial Sloane Kettering Cancer Center to not list a new colon cancer medication, called Zaltrap, due to the high cost and clinical similarity to a lower priced alternative. This type of decision (whilst similar to the formal processes carried out by PHARMAC in New Zealand) is not beholden to any formal regulatory body in the US. This gives individuals more autonomy over the medications available in the country, though at a higher cost because of lack of regulation. However, aside from the ‘slim’ 25 million people in the US without health insurance coverage, most patients do not directly incur the cost of their own healthcare as costs are deferred to third parties such as Medicaid or insurance companies.

Between the US and New Zealand, we have two very different ideologies behind two vastly divergent approaches to managing pharmaceuticals. How will this translate into a functional agreement when TPP negotiations come to a close? We should clearly elucidate the ethical issues that are continually emerging due to the TPP. We are faced with meeting compromise between two seemingly ideologically conflicting pharmaceutical systems.
The political environment has more power than philosophical reasoning in both these countries democratic systems. The goals of medicine and principles of ethics cannot be held paramount in this situation because interests outside of healthcare hold equal weight. In itself, this presents a uniquely global ethical dilemma. In bioethics, (rightly or wrongly) we utilize the four principles of autonomy, justice, beneficence and non-malfeasance to inform our judgments. Within a multi-state free trade agreement such as the TPP there are other values of equal weight, such as WTO goals of trade liberalization and longevity of economic policy.
The US Business Coalition for TPP has been formed to represent the interest of major segments of the US economy. Pharmaceutical interests in the coalition include the big names like Pfizer, GlaxoSmithKline, and AdvaMed, as well as the Society of Chemical Manufacturers and Affiliates (SOCMA). How big should the voice of these interests be? Should it overshadow that of PHARMAC’s desire to regulate pharmaceutical use in New Zealand?
In working toward a comfortable solution for both the US and New Zealand in the pharmaceutical component of TPP, key policy aims for each country have emerged. New Zealand aims to expand its export of agricultural goods to strengthen its vital economic interest- dairy. According to a January 2013 Congressional Research Service (CRS) Report, the US has previously shielded its dairy market from New Zealand. Much has been made of the US potentially removing restrictions and allowing New Zealand market access. Negotiation speculation in the CRS report indicates New Zealand may lessen regulation carried out by PHARMAC in return for access to the US Dairy market.
The impacts of economic globalization on healthcare are not clearly understood, and whilst we roughly estimate these impacts in dramatically different countries, these are hard to determine with less developmental gaps. What is certain is that in this increasingly global community, trade agreements will become pertinent to the access and supply of not only pharmaceuticals, but to healthcare overall. This can be advantageous or detrimental depending on how an agreement is constructed and what end of it you reside on.
Just exactly when the agreement might be formally agreed upon depends significantly on whether or not it is ‘fast tracked’ (Trade Promotion Authority- formerly known as fast-track- is a congressional trade agreement negotiation system.) to avoid potentially debilitating alteration by the US Congress. The ability of US Congress to make adjustments has seen wariness on the part of other participatory countries that are trying to seek assurances this process will be averted via the fast-track method. According to US President Barack Obama, “the TPP will boost our economies, lowering barriers to trade and investment, increasing exports, and creating more jobs for our people.” However, the divisive political climate of the US government may make it difficult for the proposal to enter fast track status. This will mean it may be off the table until after TPA has passed, or the political environment somewhat stabilizes.
The TPP provides an excellent opportunity for international collaboration on pharmaceuticals and healthcare issues. Both the US and New Zealand have systems that can improve in some aspects. For the US, calls for formal limited AMA or other industry regulation might be the only politically palatable possibility. Similarly in New Zealand, some limited increase in price competition would result in benefits to patient consumers without infringing on the current regulatory body. What will be most interesting to follow in this emerging issue are just how flexible principles in each country and industry will be, and what is worth compromising for.
Further Reading:
On PHARMAC:
On the TPP and USA-NZ relations:
Article Details

This work is licensed under a Creative Commons Attribution 4.0 International License.